
Guillain-Barre Syndrome physiotherapy Brisbane southside.
What is Guillain-Barre Syndrome?
Guillain-Barre syndrome (GBS) is a rare but serious autoimmune disorder that affects the peripheral nervous system. It often begins with weakness and tingling in the legs and can progress to muscle weakness or paralysis. It can develop suddenly and progress rapidly or gradually over weeks. The exact cause is unknown, but its often triggered by infections, such as respiratory or gastrointestinal infections.
What are the common symptoms of Guillain-Barre Syndrome?
Common symptoms include:
How is Guillain-Barre Syndrome diagnosed?
What is the treatment for Guillain-Barre Syndrome?
Physiotherapy plays a vital role in the management and recovery of individuals with Guillain-Barre syndrome (GBS). GBS can lead to muscle weakness, loss of coordination and balance, and reduced mobility, and physiotherapy can help address these issues and facilitate the patient's recovery. Here are some ways in which physiotherapy can be beneficial after a GBS diagnosis:
This information provides a general overview of Guillain-Barre syndrome. If you or a loved one has questions about Guillain-Barre Syndrome and how our physiotherapists might be able to help please call us on 07 3706 3407 or email [email protected]. We would love to work with you! We are happy to accept CDMPs and NDIS patients.
Guillain-Barre syndrome (GBS) is a rare but serious autoimmune disorder that affects the peripheral nervous system. It often begins with weakness and tingling in the legs and can progress to muscle weakness or paralysis. It can develop suddenly and progress rapidly or gradually over weeks. The exact cause is unknown, but its often triggered by infections, such as respiratory or gastrointestinal infections.
What are the common symptoms of Guillain-Barre Syndrome?
Common symptoms include:
- Progressive muscle weakness
- Tingling sensations
- Loss of reflexes
- Paralysis
- Difficulty breathing
How is Guillain-Barre Syndrome diagnosed?
- Medical History: A doctor will take a detailed medical history and perform a physical examination.
- Electromyography (EMG) and Nerve Conduction Studies: These tests can help assess nerve function and confirm the diagnosis.
- Cerebrospinal Fluid Examination: A lumbar puncture may be done to examine the cerebrospinal fluid for abnormalities.
What is the treatment for Guillain-Barre Syndrome?
- Intravenous Immunoglobulin (IVIG) and Plasma Exchange (Plasmapheresis): These are common treatments to reduce the severity and duration of symptoms by modulating the immune response.
- Supportive Care: Patients may require hospitalization for close monitoring of respiratory function and other complications.
- Physical Therapy: Rehabilitation plays a crucial role in recovering strength and mobility.
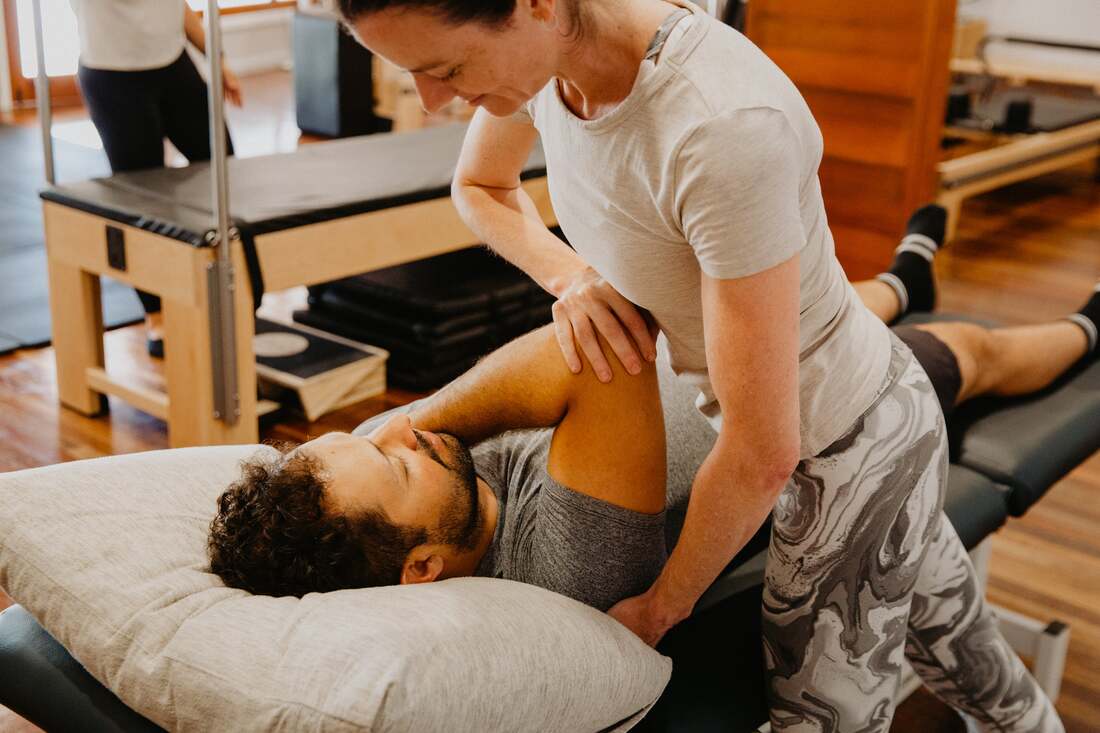
Physiotherapy plays a vital role in the management and recovery of individuals with Guillain-Barre syndrome (GBS). GBS can lead to muscle weakness, loss of coordination and balance, and reduced mobility, and physiotherapy can help address these issues and facilitate the patient's recovery. Here are some ways in which physiotherapy can be beneficial after a GBS diagnosis:
- Muscle Strengthening: GBS often results in muscle weakness and atrophy. Physiotherapy can include exercises and resistance training to help rebuild and strengthen muscles that have become weak.
- Range of Motion Exercises: GBS can cause stiffness and reduced joint mobility. Physiotherapists can guide patients through range of motion exercises to improve joint flexibility and prevent contractures (permanent shortening of muscles or tendons).
- Gait Training: Many individuals with GBS experience difficulty walking due to muscle weakness and balance issues. Physiotherapists can provide gait training to help patients regain their ability to walk safely and efficiently.
- Balance and Coordination Training: GBS can affect coordination and balance. Physiotherapy can include exercises and techniques to enhance balance and coordination, reducing the risk of falls.
- Pain Management: Some individuals with GBS may experience pain or discomfort, particularly during the recovery process. Physiotherapists can provide pain management strategies and modalities to alleviate pain.
- Breathing Exercises: In severe cases of GBS, respiratory muscles can be affected, leading to difficulty breathing. Physiotherapists can teach breathing exercises to improve lung function and help prevent respiratory complications.
- Adaptive Devices: Physiotherapists can assess the need for assistive devices like walkers, wheelchairs, or braces and provide guidance on their proper use.
- Patient Education: Physiotherapists educate patients about their condition, the importance of compliance with exercises, and strategies to prevent complications.
- Progress Monitoring: Physiotherapists continually assess the patient's progress and adjust the treatment plan accordingly, ensuring that therapy aligns with the patient's changing needs.
- Psychosocial Support: Dealing with GBS can be emotionally challenging. Physiotherapists often provide emotional support and encouragement to patients, helping them maintain a positive attitude throughout their recovery.
This information provides a general overview of Guillain-Barre syndrome. If you or a loved one has questions about Guillain-Barre Syndrome and how our physiotherapists might be able to help please call us on 07 3706 3407 or email [email protected]. We would love to work with you! We are happy to accept CDMPs and NDIS patients.

|
|

|